

How to Test for Insulin Resistance
Why Standard Tests Miss It and What to Ask For
Why Standard Tests Miss Insulin Resistance
Insulin Resistance Is Not Diabetes - But It Can Lead There
How to Test for Insulin Resistance: Every Test Compared

Fasting Glucose
HbA1C
Oral Glucose Tolerance Test (OGTT)
Fasting Insulin
HOMA-IR (Homeostatic Model Assessment)
C-Peptide
Triglycerides
Waist-to-Height Ratio: A Free Self-Assessment
The Insulin Glucose Challenge: The Most Accurate Test for Insulin Resistance

By far, the most valuable test for insulin resistance, hyperinsulinemia, and other blood sugar dysregulations is the insulin assay with oral glucose tolerance test. We frequently order this test at our clinic – we call it the Insulin Glucose Challenge in our practice.
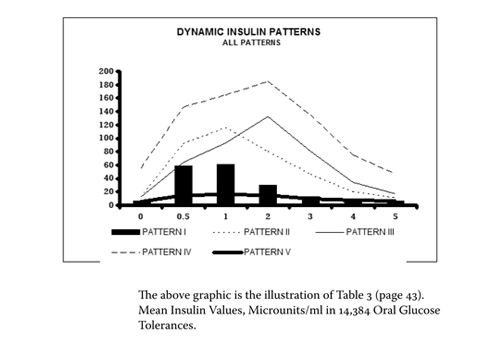
Dr. Joseph Kraft was a pathologist who completed over 3,000 autopsies and found atherosclerosis in every person over 40, at which point he became interested in how this developed. He found that the slow development of atherosclerosis was linked primarily to insulin resistance and hyperinsulinemia. Dr. Kraft ran the insulin assay with oral glucose tolerance test on 14,384 patients and published his groundbreaking results – data we can use today to understand metabolic health decades before diabetes develops.
This test uses the same glucose tolerance test infrastructure as standard medical practice – the only difference is that insulin is measured alongside glucose at each interval. It is not an alternative or experimental procedure. It is, however, an under-researched test: formal academic research has not kept pace with its clinical utility, and it deserves wider adoption.
How Does the Insulin Glucose Challenge Work?
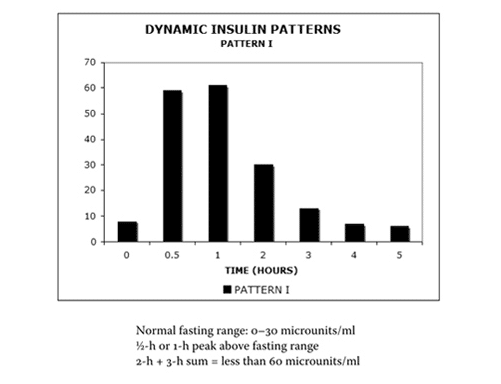
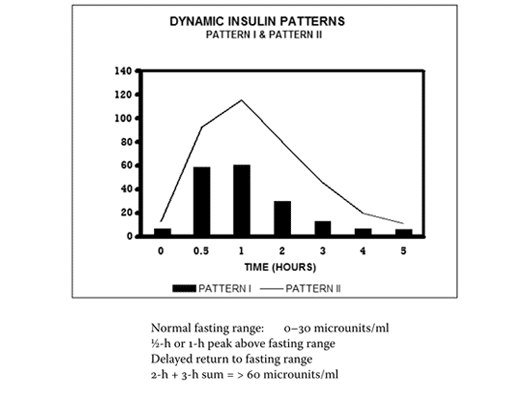
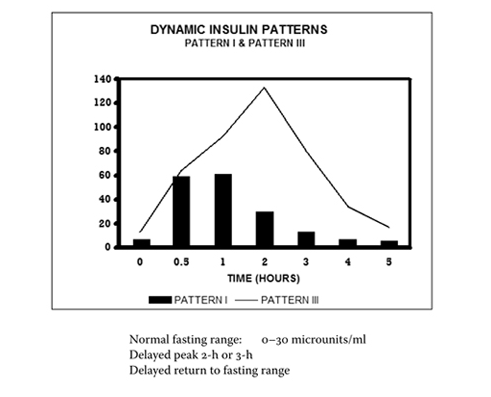
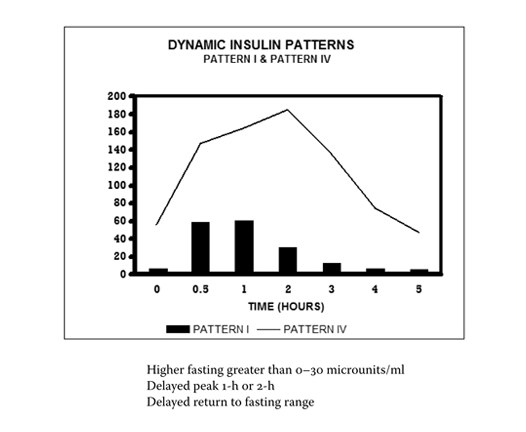
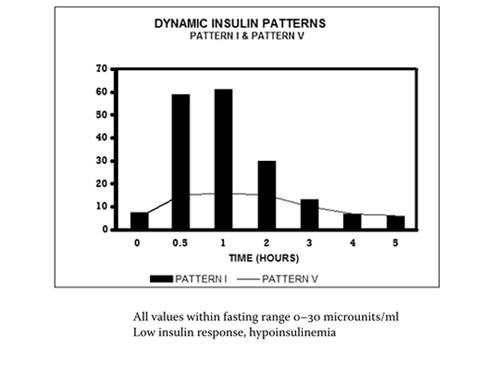
The Kraft Insulin Patterns: Stages of Insulin Resistance
(Reference: J. R. Kraft, 2011)
What Happens When You Come In for Insulin Resistance Testing
1
Case review
Your naturopathic doctor reviews your full health history, symptoms, and any previous testing. This detailed conversation is the foundation of accurate assessment - it determines which tests will be most informative for your individual situation.
2
Clinical assessment.
Based on your history and symptoms, your ND selects the appropriate tests. For patients who want a deep dive into their insulin dynamics, or whose fasting levels appear normal, the Insulin Glucose Challenge is typically recommended. For a simpler screen, a fasting insulin with HOMA-IR calculation may be sufficient.
3
Test ordering
A comprehensive insulin resistance panel typically includes: the Insulin Glucose Challenge (or HOMA-IR), along with HbA1c, a lipid panel, liver enzymes, and hs-CRP. These companion tests assess related metabolic markers - lipid health, liver function, and systemic inflammation - that are important for the complete clinical picture.
4
Results review
Your naturopathic doctor reviews the results with you, explains your insulin pattern, and creates a personalized plan based on what the testing reveals. Clinical interpretation is part of the service - you are not left with a lab printout to decipher on your own.
Frequently Asked Questions About Insulin Resistance Testing
Getting Tested for Insulin Resistance in Canada
Why Early Testing Matters: What Insulin Resistance Does Over Time
Meet our medical director, Dr Fiona Mcculloch, ND
