The American Thyroid Association has updated their guidelines for the management of thyroid concerns in pregnancy, the details of which were published in the journal Thyroid this past month. Many of us who work in the field of fertility have long been aware of research suggesting that ranges for TSH should be lower in pregnancy. It is truly great to see that this has been formally recognized. Although these were guidelines were written for pregnancy, I also apply these to women with fertility concerns who are preparing for pregnancy. Prevention is always best when it comes to avoiding miscarriage.
Thyroid disease is very common in pregnancy. One of the reasons is that one of the main thyroid hormones (free T4) decreases in pregnancy. Another reason is that TBG (thyroxine binding globulin) increases during pregnancy – TBG is a hormone that binds to the circulating thyroid hormone, making it unavailable to act on receptors. This aggravates cases of hypothyroidism by binding up the thyroid hormone that would normally be available to work in the body.
Hypothyroidism Symptoms Include:
- Difficulty losing weight despite reducing caloric intake and exercising
- Feeling cold
- Constipation
- Dry Skin
- Hair Loss
- Depression or Irritability
- List Item
- Sleeping Problems
- Difficulty concentrating or poor memory
- Brittle Nails
- Decreased Libido
hCG, the pregnancy hormone, has a profound effect on thyroid function too. Normally in pregnancy, hCG causes TSH (Thyroid stimulating hormone) to decrease. TSH is produced by the pituitary gland and causes the thyroid gland to make thyroid hormones. So in a healthy pregnancy, we expect a woman to have a lower TSH than she usually would . This makes high levels of TSH in pregnancy to be of even more concern and gives us a lower “normal” reference range for pregnancy. When TSH levels are high, this indicates that the thyroid function is low, as the pituitary is attempting to stimulate more thyroid hormone production from the thyroid gland.
Autoimmune thyroiditis is very common in pregnancy as well. 1 in 10 pregnant women will develop antibodies to the thyroid. Hypothyroidism develops in 16% of women with thyroid antibodies. Thyroid antibodies are also associated with lower success rates in IVF cycles, and increased miscarriage rates, even if there is no hypothyroidism in the patient. Postpartum thyroiditis can occur in around 50% of women who develop antibodies during pregnancy.
As you can see, thyroid conditions are a very common health problem, and have great impact on pregnancies and fertility. Not only is thyroid disease related to miscarriage, but subclinical hypothyroidism or positive thyroid antibodies can impact the brain development of the fetus and have been linked to poor intellectual development in the baby. Hyperthyroidism is related to miscarriage and a host of problems such as intrauterine growth restriction. So this is an issue we must take seriously!
The New Guidelines Suggest the Following:
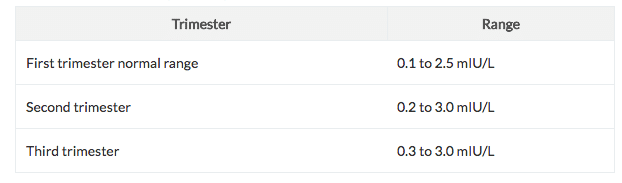
Trimester specific tighter ranges for TSH
However, in my practice, I have seen that below 2.0 is a better target range. I also like to see the free T4 and free T3 at the top of the range, especially if symptoms of hypothyroidism remain.
- Women who are already receiving thyroid replacement therapy should increase their dose by 25% to 30% when they become pregnant.
- The total amount of iodine should be 250 ug from all dietary and supplemental sources.
- Monitoring is important to ensure that women with hypothyroidism or subclinical hypothyroidism are not at risk. TSH should be measured once every 4 weeks until 16 to 20 weeks’ gestation and at least once between 26 and 32 weeks’ gestation.
Basic nutrition for thyroid in fertility programs and in pregnancy
Of note, although our salt is iodized in developed countries, there is a growing deficiency of iodine. This is because the iodine in our salt supply is not well absorbed and utilized. In pregnancy, there is a 50% increase in iodine requirements. So, choose a prenatal with some iodine content, usually around 150-200ug per day. Do not exceed 500mcg total intake daily, as this can pose an increased risk for hypothyroidism. For patients who have autoimmune thyroiditis or hashimoto’s disease, iodine may actually exacerbate these conditions so do be cautious.
- Selenium should be part of a prenatal vitamin
Several studies have shown that selenium decreases the levels of thyroid antibodies (anti thyroglobulin (anti TG) and anti thyroidperosidase (anti TPO). A randomized controlled trial found that supplementing with 200mcg of selenium daily during pregnancy and the post partum period reduced the incidence of postpartum thyroiditis in women who were positive for thyroid antibodies. 55 mcg should suffice as prevention in healthy women.
Perinatal thyroid disease is very common and new research is rapidly emerging on this topic. Thyroid disease affects fertility, pregnancy, maternal and fetal health. Women should optimally try to establish healthy thyroid function before conceiving: this way many concerns can be prevented, and the health of both moms and babies will be protected.
References
- Selenium Supplementation in Patients with Autoimmune Thyroiditis Decreases Thyroid Peroxidase Antibodies Concentrations JCEM 2002 87: 1687-1691
- Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and Postpartum. The American Thyroid Association Taskforce on Thyroid Disease During Pregnancy and Postpartum. THYROID Volume 21, Number 10, 2011
- Dietary Iodine: Why Are So Many Mothers Not Getting Enough? Renner R 2010. Environ Health Perspect 118:a438-a442. Increased prevalence of thyroid antibodies in euthyroid women with a history of recurrent in-vitro fertilization failure Hum. Reprod. (2000) 15(3): 545-548