
How to Lengthen Your Luteal Phase Naturally

If you have been tracking your basal body temperature and noticed that your post-ovulation phase is shorter than 12 days, or if a doctor has told you that you have a luteal phase defect, you are right to take it seriously. A short luteal phase — clinically called a luteal phase defect — means the time between ovulation and your next period is not long enough for the endometrium to fully prepare for implantation. Without a healthy luteal phase implantation can’t happen, and so effective luteal phase defect treatment is crucial to restore healthy fertility. This page explains the causes of a short luteal phase — including thyroid dysfunction, ovulation quality, and PCOS — how it is diagnosed, and the evidence-based supplements and treatments that support luteal phase function.
By Dr. Fiona McCulloch, ND author of 8 Steps to Reverse Your PCOS
Struggling with a short luteal phase? Our naturopathic fertility team can help identify the cause. Book a fertility assessment
If You've Tried Supplements and Your Luteal Phase Is Still Short
You may have already tried the standard advice: prenatal vitamins, Vitex from a health food store, vitamin B6, carefully timed intercourse, ovulation predictor kits. Perhaps a doctor suggested Clomid, or told you to wait 12 months before investigating further. These approaches are not wrong — but they share a common limitation. They skip the diagnostic step. There really is no base protocol for luteal phase supplements, because the cause of a short luteal phase matters. Some supplements target circulation, others support thyroid function, and others improve ovulation quality. If you have been supplementing without knowing the underlying cause, the protocol may not have been addressing your specific situation.
Fertility struggles carry an emotional weight that clinical information alone does not capture. The grief of another cycle that did not result in pregnancy, the isolation of a diagnosis that most friends have never heard of, the pressure of feeling like your body is not doing what it should — these experiences are common among patients navigating a short luteal phase, and they are valid.
A short luteal phase is a symptom, not a standalone condition. It can be caused by thyroid dysfunction, poor ovulation quality, or PCOS-related anovulation. Identifying the underlying cause is the first step toward effective treatment — because the cause determines which interventions will actually work. As Dr. Fiona McCulloch explains: “Knowing what the cause is is very helpful and important. The supplements really are all situational.”
What a Luteal Phase Assessment Involves
1
Clinical interview
We review your symptoms, cycle history, BBT charts, prior testing, PMS symptoms, and spotting patterns. If you have been supplementing already, that information is valuable — it tells us what has and has not responded.
2
2
Targeted testing
We test estrogen and progesterone levels in the luteal phase, a comprehensive thyroid panel, and other relevant labs. These specific tests at the right time in your cycle identify whether the issue is ovulation quality, thyroid function, or another factor.
3
Individualized protocol
Once the underlying cause is identified, we create a targeted plan: supplements matched to your specific cause, bioidentical progesterone if indicated, and lifestyle modifications where relevant. There is no one-size-fits-all protocol.
4
Follow-up and monitoring
Most patients see luteal phase improvement within one to three months of targeted treatment. We monitor progress through follow-up hormone testing to confirm the protocol is working.
Initial consultations are available virtually. Lab requisitions are completed at a local laboratory. Naturopathic visits are covered by most employer extended health plans, and we offer direct insurance billing.
Check out our Fertility program
What Causes a Short Luteal Phase?
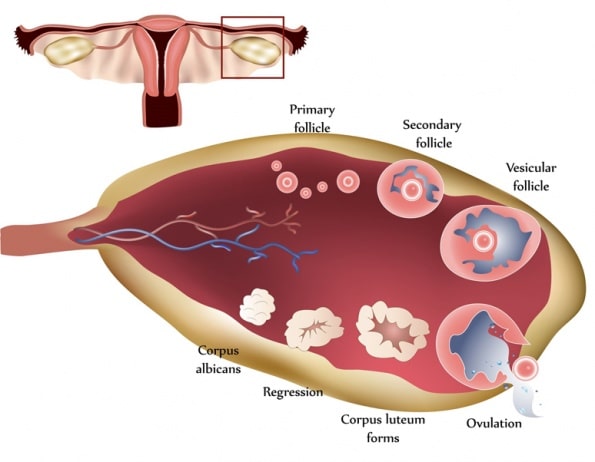
Poor Ovulation Quality and Corpus Luteum Function
The corpus luteum forms from the follicle after ovulation and produces the progesterone that maintains the endometrial lining during the luteal phase. If ovulation is weak or the corpus luteum is insufficient, progesterone production drops and the luteal phase shortens. The metabolic demands on the corpus luteum are extraordinary — it consumes 2 to 6 times more oxygen per unit weight than the liver, kidney, or even the heart.1 This is why circulation and mitochondrial support are central to luteal phase treatment: the corpus luteum requires adequate blood flow and oxygen to produce progesterone at the levels needed for implantation.
Thyroid Dysfunction
Thyroid hormones work synergistically with follicle-stimulating hormone to develop healthy granulosa cells. Thyroid hormones have also been found to augment steroidogenesis from granulosa and large luteal cells.2 This means that even subclinical thyroid dysfunction — where standard lab values may appear “normal” — can impair corpus luteum function and reduce progesterone production. If you have been told your thyroid is fine but your luteal phase is still short, a more detailed thyroid assessment using functional reference ranges may reveal a contributing factor that standard testing missed.
PCOS and Progesterone Deficiency
In PCOS, a short luteal phase may reflect a deeper issue. Many patients with PCOS experience partial or complete anovulation, meaning progesterone production is not just reduced — it can be absent entirely. Ovulation and egg quality determine progesterone levels in PCOS. If you are not ovulating consistently, the corpus luteum does not form, and progesterone is not produced. This is a fundamentally different mechanism than a weak corpus luteum, and it requires a different treatment approach — one that addresses ovulation quality and the underlying PCOS factors driving anovulation. Learn more about PCOS and infertility or PCOS naturopathic treatment.
Significant stress can also suppress ovulation by downregulating reproductive signaling through the hypothalamus — the brain effectively conserves reproductive energy under prolonged stress. This is a brain-level mechanism, distinct from direct hormonal effects, and is identifiable through laboratory testing.
How Is a Short Luteal Phase Diagnosed?
- Basal body temperature charting — A luteal phase shorter than 12 days on a BBT chart indicates that the corpus luteum has degenerated prematurely. Luteal phase temperature should be high and steady; instability or a premature drop suggests poor corpus luteum quality.
- Clinical signs — Spotting or bleeding in the luteal phase, significant PMS symptoms, and bleeding before the expected onset of menses are assessed during the clinical interview.
- Serum progesterone — A progesterone level below 20 ng/mL obtained 7 days after ovulation indicates poor function of the luteal cells. The timing of this test matters — progesterone must be measured at the right point in the cycle to be meaningful.
- Estrogen testing — Estrogen is tested alongside progesterone in the luteal phase to evaluate the overall hormonal environment supporting implantation.
- Thyroid panel — A comprehensive thyroid assessment identifies subclinical dysfunction that may be impairing corpus luteum function, even when standard screening appears normal.
These tests are targeted and specific — not another round of bloodwork without direction. They identify the underlying cause so the protocol addresses your situation, not a generic checklist. Read more about how we approach hormone health.
Luteal Phase Supplements: Evidence-Based Options
There is no base protocol for luteal phase supplements. The cause of your short luteal phase determines which supplements apply. Some target circulation and blood flow to the corpus luteum, others support thyroid function, and others improve ovulation quality and mitochondrial health. The supplements listed below have evidence for supporting luteal phase function — but which combination is appropriate for you depends on what your assessment reveals. This is why testing before supplementation matters.
Supplements for the Entire Cycle
- Maritime pine bark extract (50 mg 3 times a day) — Enhances circulation, reduces clotting, and increases growth hormone secretion to support function of the corpus luteum.3
- Vitamin B6 as pyridoxal-5-phosphate (100 mg/d as part of a B-complex) — Modulates expression of receptors to hormones and progesterone.4 Vitamin B complex also supports adrenal health and stress responses.
- Melatonin (1.5–3 mg at bedtime) — Increases progesterone production in luteal cells and supports growth hormone secretion.5–7
- Vitamin C (750 mg/d) — Improves progesterone levels and has been shown to increase fertility in women with luteal phase defect.8
- Magnesium glycinate (400 mg/d) — Required during the luteal phase because of increased progesterone synthesis demands.9
- Omega-3 fatty acids (approximately 1200 mg EPA and 800 mg DPA daily) — Essential for follicle structure and function. Directly increase progesterone secretion and enhance uterine and ovarian blood flow by improving the prostacyclin-to-thromboxane ratio.10–12
- Zinc picolinate (30 mg/d) — Increases insulin-like growth factor 1 and growth hormone. Zinc deficiency may impair formation of the corpus luteum.13,14
- Coenzyme Q10 (800 mg/d) or ubiquinol (300 mg/d) — Supports mitochondrial function and biosynthesis in endoplasmic reticulum for luteal cell development and function.15
Supplements for the Luteal Phase Only
- Vitex agnus-castus (170 mg of a 6:1 extract of Vitex fruit daily on rising) — Boosts progesterone production. Taken during the luteal phase only, on rising — the timing specificity is clinically important.16,17
Which combination of these supplements applies to your situation depends on whether the underlying issue is circulation, thyroid function, ovulation quality, or another factor. Our assessment identifies the cause so the protocol targets your specific situation.
Bioidentical Progesterone for Fertility
For patients trying to conceive with a significant luteal phase defect, cyclic bioidentical progesterone can provide a safety net. As Dr. Fiona McCulloch explains: when pregnancy can be difficult to achieve for some patients, we do not want to take any chances. Cyclic progesterone is especially considered for patients with prior miscarriages, known low progesterone levels, luteal phase spotting, or difficulty maintaining BBT temperatures. Increased serum progesterone levels improve blood flow to the corpus luteum and promote changes in the endometrium that support implantation.1 Bioidentical progesterone is always offered as a patient choice — it is an option, not a requirement.
Progesterone is a required hormone for implantation. Most patients trying to conceive tolerate bioidentical progesterone well. There may be a brief adjustment period of a few days, after which it is well tolerated. Our naturopathic doctors have experience with various progesterone forms and with acclimatizing patients to cyclic progesterone therapy. For more on progesterone’s role in early pregnancy, see progesterone and miscarriage.
Bioidentical progesterone is available by prescription from our licensed naturopathic doctors. For patients trying to conceive with a significant luteal phase defect, cyclic progesterone provides a safety net while the underlying cause is being addressed. Learn about our Fertility Program→
Understanding the Corpus Luteum: Why It Matters for Your Luteal Phase
The formation of the corpus luteum is the culmination of a long biological process. By the end of the follicular phase, the luteinizing hormone surge ejects the oocyte and transforms the remaining follicle into the corpus luteum. Small and large luteal cells form from theca and granulosa cells, respectively. The large luteal cells produce 6 to 8 times the progesterone of the small luteal cells and aromatize androgens to estrogen. Membranes of luteal cells sit in proximity to capillaries, which supports the extraordinarily high metabolism of the corpus luteum — consuming 2 to 6 times more oxygen per unit weight than the liver, kidney, or even the heart.1
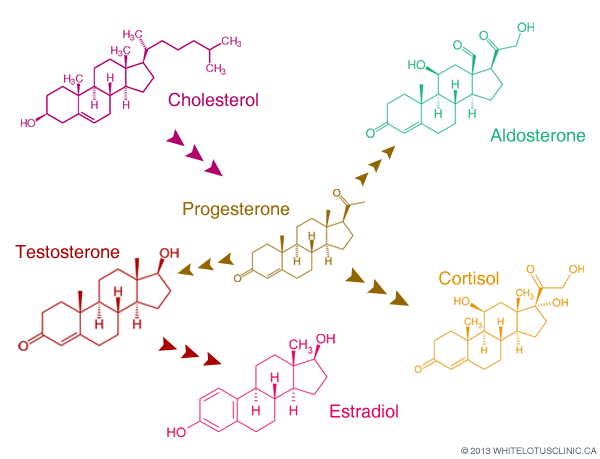
Production of progesterone depends on mitochondrial function in the luteal cells and a host of hormonal factors, including luteinizing hormone, growth hormone, insulin-like growth factor 1, prostaglandin E2, and prostacyclin.1 It also depends on the availability of its precursors cholesterol and pregnenolone. This is why general nutrition — a whole-foods diet with high-quality protein, healthy fats from avocados, nuts, seeds, and free-range organic eggs — provides the substrate foundation that supplements build upon. Because the menstrual cycle involves follicular development spanning months, nutrition in the year before a cycle can affect luteal phase quality.
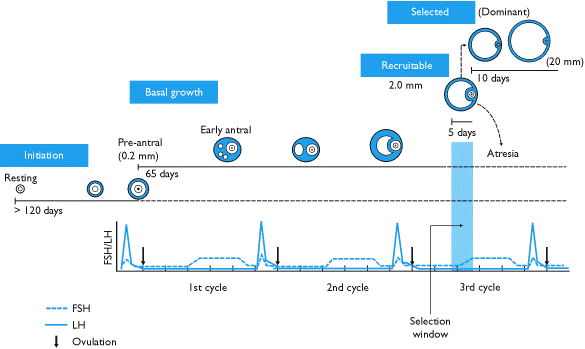
Why Starting Now Matters: The 375-Day Follicle Timeline
There is a common misconception that a follicle develops in a single menstrual cycle. In reality, the process of folliculogenesis begins around 375 days before ovulation with the recruitment of primordial follicles that have been dormant since birth. The follicle that will ovulate a year from now is being influenced by your body’s current hormonal environment today. Supporting that follicle’s development now — by correcting thyroid function, improving circulation, optimizing ovulation quality — has compounding effects on future fertility. This is not about rushing. It is about recognizing that luteal phase support is a long-term investment in follicle quality, not a single-cycle intervention.
Frequently Asked Questions About Short Luteal Phase
How long should a luteal phase be?
A healthy luteal phase is typically 12 to 14 days. If your luteal phase is consistently shorter than 12 days — as measured by basal body temperature charting — this may indicate a luteal phase defect, which is the clinical term for a short post-ovulation phase. A shorter luteal phase can reduce the window available for implantation.
Can PCOS cause a short luteal phase?
Yes. In PCOS, many patients experience partial or complete anovulation, meaning progesterone production is reduced or absent entirely. Ovulation and egg quality determine progesterone levels in PCOS. If you have PCOS and a short luteal phase, the underlying issue may be ovulation quality rather than corpus luteum function alone. Learn more about PCOS and fertility.
Can a naturopath help with luteal phase defect?
Licensed naturopathic doctors with a clinical focus in fertility assess and treat luteal phase defect through hormone testing, individualized supplement protocols, and bioidentical progesterone prescribing. At White Lotus Clinic, Dr. Fiona McCulloch has over 25 years of clinical experience in fertility and hormonal health, is a Fellow of the American Board of Naturopathic Endocrinology, and was a peer reviewer of the 2023 International PCOS Guidelines. Many of our patients are also working with a reproductive endocrinologist — naturopathic fertility care is complementary, not a replacement.
Will these supplements conflict with my fertility treatment?
Our naturopathic doctors coordinate with your fertility clinic. Supplement protocols are individualized based on your complete assessment, including any existing medications or fertility treatments. There is no generic protocol — each plan is built around the individual’s complete situation, so potential interactions are reviewed before any recommendations are made.
How much does a fertility assessment cost? Is it covered by insurance?
Naturopathic visits are covered by most employer extended health plans, and we offer direct insurance billing. Lab testing is requisitioned through standard laboratories. Supplements are a separate, self-directed cost. View current fees and insurance information.
Do I need all of the supplements listed?
No. There is no base protocol for luteal phase supplements — the cause determines which ones apply. Some target circulation, others support thyroid function, and others improve ovulation quality. An assessment identifies the underlying cause of your short luteal phase so the protocol targets your specific situation rather than applying every option.
How long until my luteal phase gets longer?
Most patients see luteal phase improvement within one to three months of targeted treatment. We monitor progress through follow-up hormone testing to confirm that the underlying cause is being addressed and the luteal phase is responding.
I've already tried Vitex and B6 — why didn't they work?
If supplements alone haven’t improved your luteal phase, the underlying cause likely hasn’t been identified. A thyroid issue, ovulation quality problem, or other factor may be preventing the supplements from working. An assessment identifies the root cause so the protocol targets the actual problem — not just the symptom. Prior supplement use is valuable diagnostic information, not a failure.
Is bioidentical progesterone safe while trying to conceive?
Progesterone is a required hormone for implantation and early pregnancy. Most patients trying to conceive tolerate bioidentical progesterone well. There may be a brief adjustment period of a few days — after which it is well tolerated by most patients. Bioidentical progesterone is always offered as a patient choice, and our naturopathic doctors have experience with various progesterone forms and acclimatization protocols. Learn about cyclic progesterone therapy.
Can I do this remotely if I'm not in Toronto?
Initial consultations are available virtually. but you have to be in Ontario at the time of your appointment. Lab requisitions can be completed at a local laboratory near you. Follow-up appointments can also be conducted by video.
Do I have to commit to ongoing naturopathic care?
You can book a single assessment. If results warrant a protocol, we will recommend a plan with a follow-up timeline — but the decision to continue is yours. There is no commitment beyond the initial visit.
Can you fix a short luteal phase?
A short luteal phase can often be improved by identifying and addressing the underlying cause — whether that is thyroid function, ovulation quality, PCOS, or another factor. With targeted treatment, most patients see improvement within one to three months. The key is determining why the luteal phase is short, because the cause determines the treatment.
Meet our medical director, Dr. Fiona McCulloch, ND
Dr. Fiona McCulloch is a peer reviewer of the 2023 International Evidence-Based Guidelines for the Assessment and Management of PCOS. She is the published author of 8 Steps to Reverse Your PCOS, and a former board member of the Endocrinology Association of Naturopathic Physicians. With over 25 years of clinical practice and a clinical focus in fertility, PCOS, and hormonal health, Dr. McCulloch founded White Lotus Clinic in Toronto.
Our naturopathic doctors have extensive experience prescribing bioidentical progesterone for fertility, including cyclic progesterone and various progesterone forms. Every protocol is individualized based on your assessment — there is no one-size-fits-all approach to luteal phase treatment.

What Luteal Phase Support Can Look Like
With the right assessment and individualized support, many patients move from uncertainty about their luteal phase to having a clear understanding of the cause and a targeted plan. The underlying factors that affect your luteal phase — thyroid function, ovulation quality, hormonal balance — are assessable and addressable. The goal is not just to lengthen the luteal phase by a few days, but to understand and support the broader hormonal picture. As Dr. Fiona McCulloch notes, the causes of a short luteal phase may also be impacting other elements of health, fertility, and hormones — so addressing them improves the whole picture, not just one metric. Learn more about our naturopathic fertility program.
Book a Fertility or Hormone Assessment
Dr. Fiona McCulloch and our naturopathic team assess luteal phase function through comprehensive hormone testing — including estrogen and progesterone levels, thyroid panels, and targeted labs — to identify the underlying cause of a short luteal phase. We create individualized protocols based on your results, because the cause determines the treatment. Most patients see improvement within one to three months.
Learn more about our Fertility program →
Naturopathic visits are covered by most employer extended health plans. Virtual consultations available.
References
- Niswender GD, Juengel JL, Silva PJ, Rollyson MK, McIntush EW. Mechanisms controlling the function and life span of the corpus luteum. Physiol Rev. 2000;80(1):1-29.
- Datta M, Roy P, Banerjee J, Bhattacharya S. Thyroid hormone stimulates progesterone release from human luteal cells by generating a proteinaceous factor. J Endocrinol. 1998;158(3):319-325.
- Buz’Zard AR, Peng Q, Lau BH. Kyolic and Pycnogenol increase human growth hormone secretion in genetically-engineered keratinocytes. Growth Horm IGF Res. 2002;12(1):34-40.
- Tully DB, Allgood VE, Cidlowski JA. Modulation of steroid receptor–mediated gene expression by vitamin B6. FASEB J. 1994;8(3):343-349.
- Taketani T, Tamura H, Takasaki A, et al. Protective role of melatonin in progesterone production by human luteal cells. J Pineal Res. 2011;51(2):207-213.
- Durotoye LA, Webley GE, Rodway RG. Stimulation of the production of progesterone by the corpus luteum of the ewe by the perfusion of melatonin in vivo and by treatment of granulosa cells with melatonin in vitro. Res Vet Sci. 1997;62(2):87-91.
- Nassar E, Mulligan C, Taylor L, et al. Effects of a single dose of N-acetyl-5-methoxytryptamine (Melatonin) and resistance exercise on the growth hormone/IGF-1 axis in young males and females. J Int Soc Sports Nutr. 2007;4:14.
- Henmi H, Endo T, Kitajima Y, Manase K, Hata H, Kudo R. Effects of ascorbic acid supplementation on serum progesterone levels in patients with a luteal phase defect. Fertil Steril. 2003;80(2):459-461.
- Facchinetti F, Borella P, Valentini M, Fioroni L, Genazzani AR. Premenstrual increase of intracellular magnesium levels in women with ovulatory, asymptomatic menstrual cycles. Gynecol Endocrinol. 1988;2(3):249-256.
- Zachut M, Dekel I, Lehrer H, et al. Effects of dietary fats differing in n-6:n-3 ratio fed to high-yielding dairy cows on fatty acid composition of ovarian compartments, follicular status, and oocyte quality. J Dairy Sci. 2010;93(2):529-545.
- Coyral-Castel S, Ramé C, Fatet A, Dupont J. Effects of unsaturated fatty acids on progesterone secretion and selected protein kinases in goat granulosa cells. Domest Anim Endocrinol. 2010;38(4):272-283.
- Saldeen P, Saldeen T. Women and omega-3 fatty acids. Obstet Gynecol Surv. 2004;59(10):722-730.
- Yu ZP, Le GW, Shi YH. Effect of zinc sulphate and zinc methionine on growth, plasma growth hormone concentration, growth hormone receptor and insulin-like growth factor–I gene expression in mice. Clin Exp Pharmacol Physiol. 2005;32(4):273-278.
- Hamza RT, Hamed AI, Sallam MT. Effect of zinc supplementation on growth hormone insulin growth factor axis in short Egyptian children with zinc deficiency. Ital J Pediatr. 2012;38(1):21.
- Bentinger M, Tekle M, Dallner G. Coenzyme Q: biosynthesis and functions. Biochem Biophys Res Commun. 2010;396(1):74-79.
- Ibrahim NA, Shalaby AS, Farag RS, Elbaroty GS, Nofal SM, Hassan EM. Gynecological efficacy and chemical investigation of Vitex agnus-castus L. fruits growing in Egypt. Nat Prod Res. 2008;22(6):537-546.
- Bergmann J, Luft B, Boehmann S, Runnebaum B, Gerhard I. The efficacy of the complex medication Phyto-Hypophyson L in female, hormone-related sterility: a randomized, placebo-controlled clinical double-blind study. Forsch Komplementarmed Klass Naturheilkd. 2000;7(4):190-199.